Valerio Pace
University of Perugia, Italy
Posters & Accepted Abstracts: J Sports Med Dop Stud
Biceps tendons are intra-articular but extra-sinovial structures contained in a sling formed by CHL and SGHL and representing a primary restraint from rotator interval. His main functions are elbow flexion and forearm supination, compression of HH into glenoid, humeral head depressor, shoulder stabilizer. His etiology includes instability (anterior or posterior, due to loss of soft tissue restraints, association with pulley lesions and LHB pathology), rupture (degeneration, high energies, deceleration of forearm, slap tears), inflammation (mechanical wear under coracoacromial arch, usually coexisting rotator cuff disease). Most used classification systems are Habermeyer e Walch. The medical history is characterized by pain, popping or snapping, night pain, pain with overhead activities (sports). Examination findings include tenderness at bicipital groove and positivity to Yergason test, Speed test, Lift-off test, rotator cuff strength test, impingment tests. USS and MRI are useful imaging. Conservative treatment includes rest, ice, Nsaids, physical therapy (cuff strengthening, periscapular strengthening), injections (biceps tendon sheath, subacromial, intra-articular). Operative treatment options are tenotomy or tenodesis with no significant differencies in literature. Tenotomy has the advantage of having a 90% success rate, being an easy procedure, no immobilization is needed, no need for rehab but about 70% gets Popeye deformity, weak resisted elbow flexion, mild loss of flexion and supination strength. Tenodesis has the advantage of providing better cosmetic results, restoration of strength, maintain length-tension relationship but it is also a more difficult procedure with the use of costly implants and involves a longer rehab, immobilization and a significative failure rate. Surgical techniques are represented by Post, Keyhole, Suture Anchor, Tenodesis Screw, Arthroscopic Tenodesis (Anchor, interference screw, suture to rotator interval). Proximal ruptures are often treated conservatively. Supra and Infra-Pectoral access are available. Rehab includes sling for comfort, no isolated biceps exercises for 8/52, no jerking movements, achievement of full ROMs by 2-3/52, dynamic strengthening exercises at 6-12/52, sport specific programs at 10/52, RTP 16-20/52. The management is based on multifactorial aspects including type of sport and level.
Valerio Pace has completed his MBBS at the University of Perugia. He worked as T&O SHO and Registrar at Royal National Orthopaedic Hospital (RNOH) NHS Trust between 2015 and 2017. He is currently a T&O Resident Doctor at the University of Perugia, Italy. He also has Honorary Research Contract at the Royal National Orthopaedic Hospital. He has published eight papers in reputed journals, presented at several conferences and carrying on plenty of on-going research projects.
E-mail: valeriopace@doctors.org.uk
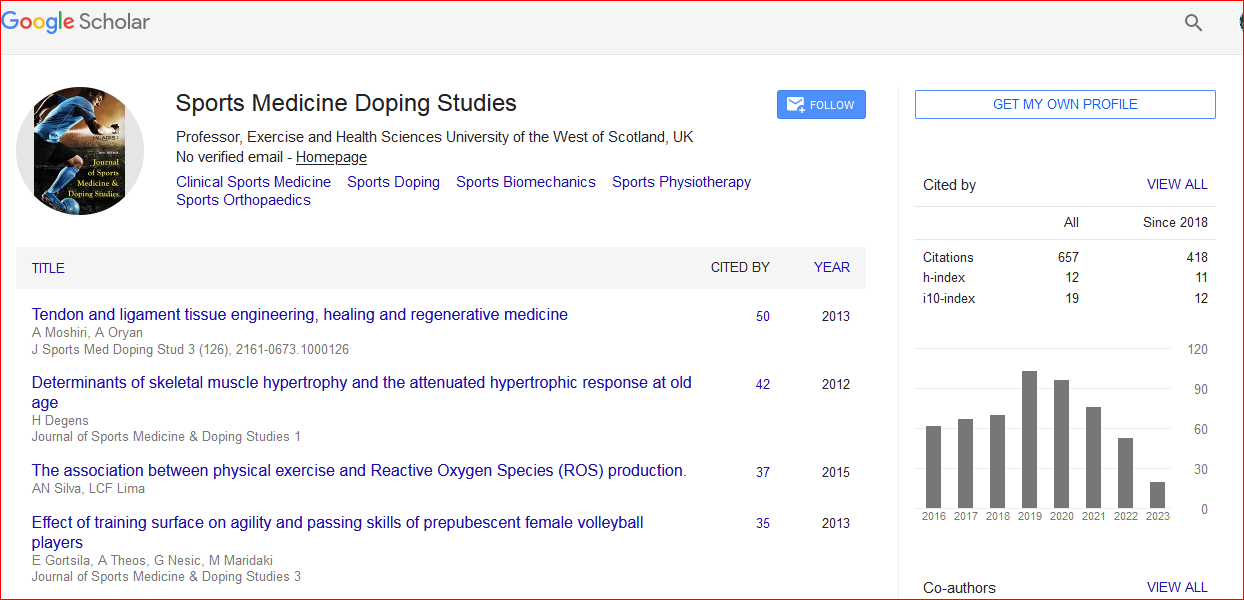
Journal of Sports Medicine & Doping Studies received 1022 citations as per Google Scholar report

 Spanish
Spanish  Chinese
Chinese  Russian
Russian  German
German  French
French  Japanese
Japanese  Portuguese
Portuguese  Hindi
Hindi 