Ibrahim Abuomira
Al-Azhar University, Egypt
Scientific Tracks Abstracts: J Sports Med Doping Stud
Introduction & Aim: Poliomyelitis first occurred nearly 6000 years ago in the time of the ancient Egyptian. Poliomyelitis is still a common condition in developing countries. Immunization has decreased the number of new patients, but still there are many patients (old polio patient). With skeletal growth, fixed soft tissue and deformities develop in the foot in poliomyelitis. Conventional operative treatment of this deformity involves corrective osteotomies, arthrodesis, extensive tissue release and tendon transfers, may result in neurovascular injury and soft tissue problems. Leg shortening and complex foot deformity are common in patients with deformity after poliomyelitis. This study aims to find out the special technique for deformity correction of the foot for restore plantigrade foot and improve ambulation. The Ilizarov method of gentle, gradual correction of this deformity has become a treatment option for poliomyelitis foot deformity. This method is considered to be safe than traditional methods of the treatment. Material & Methods: Between 1994 and 2009, a total of 25 rigidly deformed feet belonging 25 patients were studied. All cases were treated with classic ring Ilizarov fixator. The average age of the patients was 34 (range- 12 to 56) years. Ten of 25 patients underwent previous surgical intervention. The types of deformities observed before surgery were: Equinus foot 6 cases, equinovarus 4, equinovalgus 5, supinated equinovarus 2, equinocavovarus 3 and vertical calcaneus with calcaneovalgus 2 cases. In 15 cases, observed limb-length discrepancy ranged from 2 to 6 cm (the mean was 3.5 cm). Results: The mean follow-up period was 7.17 years (range 6 months to15 years). There were 6 patients who underwent correction by a closed method (bloodless technique) with the Ilizarov fixator and without any additional procedures. The open method with V-shaped osteotomy and calcaneal osteotomy was used in 5cases, supramalleolar osteotomy in 2 cases, triple and ankle arthrodesis in 3 cases and a Chopart joint arthrodesis in one. The additional procedures performed included limb lengthening in 13 cases, Achilles tendon lengthening in 8 cases, knee arthrodesis and proximal tibial lengthening in 1 case. At the time of fixator removal, a plantigrade foot was achieved in nearly all patients and the leg-length discrepancy eliminated in all cases where it was present. As compared to the preoperative status, all patients were satisfied with their gait. The correction period ranged from 2 months to 3.5 months. The mean duration of fixator usage was 4.2 months (range 3��?7) for the foot portion of the fixator and about 6.1 months (range 5��?10) for the tibial portion. In most cases, treatment time depended on consolidation of the tibial segment rather than the foot osteotomy. We observed residual varus and equinus deformities of the foot in 2 cases that were treated by repeated fixator applications. There were recurrent deformities in 2 patients who were then managed by a V-shaped osteotomy and application of the Ilizarov frame. One patient ended up with a stiff ankle and osteoarthritis and was managed by ankle arthrodesis; another patient had significant pain and was managed by physiotherapy. Complications including pin track infection were infrequent and accounted for 15% of patients; all these patients were treated with oral antibiotics. One patient had a good correction of the foot deformity by triple arthrodesis but had difficulty walking because of weakness of the quadriceps muscles and a flexion contracture of the knee (a brace was fabricated in order to keep the knee in the extended position). Another patient had a knee contracture after femoral lengthening, tibial lengthening and gradual foot deformity correction through a V-osteotomy that persisted for 1 year; this patient declined further treatment. In this study, at the time of Ilizarov removal, a plantigrade foot was achieved in 25 cases, mild residual varus and equines deformities were present in 2 cases, significant pain after removal of the frame, a stiff ankle and recurrent deformity were in one patient, respectively.
Ibrahim Abuomira is a Lecturer of Orthopedic, Al-Azhar University, Egypt. He is a Consultant in Deformity Correction and Limb Lengthening, Pediatric Orthopedic Surgery and obtained his MD from Institute Clinico Humanitus, Milano University, Italy during 2007-2010. He has received his PhD at Al-Azhar University in 2011 and is a Member of Egypt ASAMI, Member of International ASAMI and Member of American Academy for CP.
Email: ibrahim_amira2000@yahoo.com
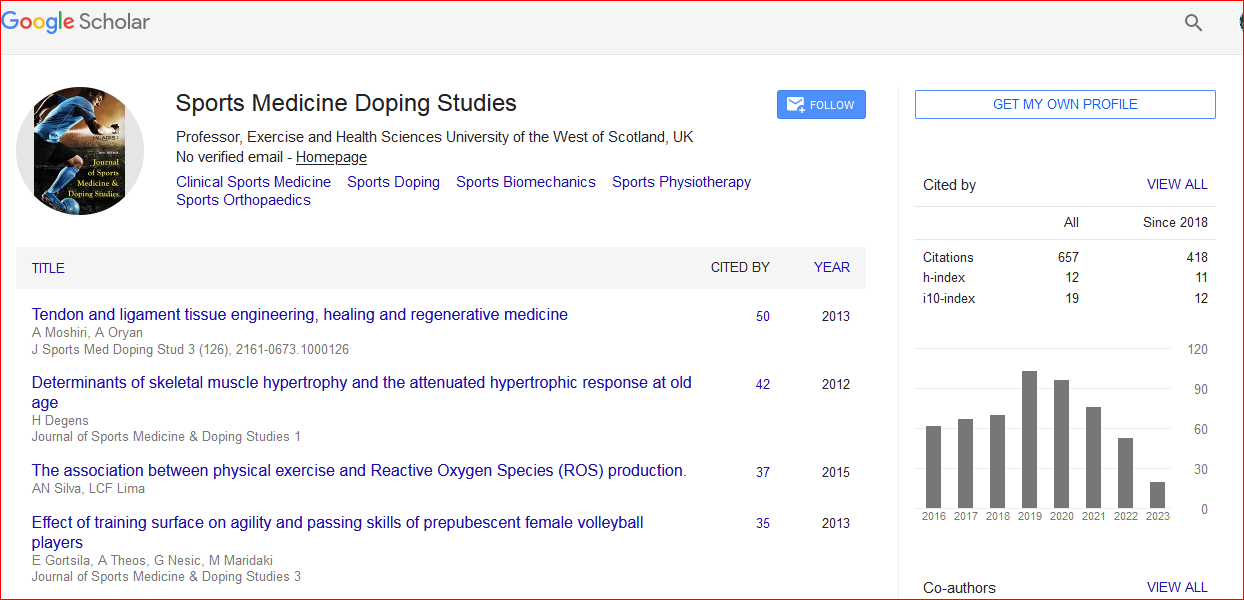
Journal of Sports Medicine & Doping Studies received 1022 citations as per Google Scholar report

 Spanish
Spanish  Chinese
Chinese  Russian
Russian  German
German  French
French  Japanese
Japanese  Portuguese
Portuguese  Hindi
Hindi 