Research Article - (2021) Volume 12, Issue 11
Received: 19-Oct-2021
Published:
16-Nov-2021
, DOI: 10.37421/2155-6113.2021.12.871
Citation: Sewale, Yihenew, Nurilign Abebe Moges, Bitew Tefere Zewedie, and Addisu Endale Gebeyew, et al. “Stunting and its Associated Factors among Human Immunodeficiency Virus Positive Children Who Receiving Anti-Retroviral Therapy in Northwest Ethiopia: Multicenter Study.” J AIDS Clin Res 12 (2021): 871.
Copyright: © 2021 Sewale Y, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction: Human immunodeficiency virus positive children are highly vulnerable for stunting and stunting is the most serious public health problems in human immunodeficiency virus-positive children who received antiretroviral therapy in the developing world particularly low and middle-income countries. Therefore, the aim of the study was to assess the magnitude of stunting and its associated factors among human immunodeficiency positive children in public Hospitals Northwest, Ethiopia.
Methods: Multicenter cross-sectional study was conducted among 372 HIV infected children. Data were collected systematically from selected participants by using interviewer administered structured and pre-tested questionnaires. We used Epi-data version 4.1 for data entery, and STATA Version 14.1 for data analysis. a p-value of <0.05 was considered to declare statistical significance with the corresponding 95% confidence interval. The goodness of fit (GOF) of the model was checked using Hosmer-Lemeshow GOF test. The p-value of the Hosmer-Lemeshow GOF test of this model is p-value greater than 0.05 which confirms that the model is correctly specified.
Results: The magnitude of stunting was found to be 45.2%, 95% CI (40.4-50.0). Being males (AOR:1.942, 95% CI:1.188, 3.175), age of the child 2-5 years old, opportunistic infections (AOR: 2.40,95%,CI: 1.61, 7.60), and fair/poor dietary diversity (AOR:1.832,95% CI:1.1280, 2.95) were found statically significant associated factors.
Conclusion: More than one-thrid of chlidern was stunted among human immunodeficiency virus-positive children received antiretroviral therapy. Therefore, early detection and treatment of opportunistic infections, control progression of HIV, educating and counseling the use of a diversified diet,and monitoring this situation was highly recommended.
Stunting • HIV • ART
ART: Antiretroviral Therapy • HIV: Human Immunodeficiency Virus • WHO: World Health Organization • AIDS: Acquired Immune Deficiency Syndrome
Stunting is inadequate energy, protein, and micronutrients to meet the basic requirements for body maintenance, growth, and development of children [1]. Globally, nearly 2.84 million children were living with human immuodeficency virus (PLWHIV), of which more than 90% were in sub- Saharan Africa in 2019 [2]. Stunting is also the most serious public health problem in the world particularly low and middle-income countries [2,3]. Both stunting and human immunodeficiency virus (HIV) are highly prevalent in the world, particularly in sub-Saharan Africa which was to be 32% [4,5]. A few studies which is conducted in Tanzania, Nigeria, and Burkina Faso also showed that stunting was more prevalent among HIV infected children than non-HIV infected children [6-8].
The prevalence of stunting was higher among HIV-infected children than non-HIV-infected children [9]. Stunting also increased the frequency and severity of the opportunistic infection, delayed recovery from disease, recurring of sickness, faltering growth, and diminished learning ability in HIV infected person [8,10],and affecting the overall clinical outcomes of HIV chronic care in ART clinics [11]. Human immunodefiency virus that induced immune impairment and enhanced contributing of infection that affect negatively the nutritional status of children which leads to undernourished through decreament of food intake, increased utilization and execretion of nutrients, mal-absorption syndrome and that increase the progression of diseases at a patient, whres as HIV infection also induced stunting by weakening of the immune system and distorted of nutrient intake, absorption and body's use of food [12].
Stunting is a significant factor affecting human immune deficiency virus care and treatment outcome particularly developing countries [13]. This problem occurred due to, stunting underlying poor nutritional status with food insecurity, poverty, and co-infections that pose a serious threat to efforts to combat HIV/AIDS by denying access of a nutrition-rich diet, hindering the chance of good health outcomes [14]. The study which is conducted in southern India showed that the magnitude of stunting among HIV-infected children receiving antiretroviral therapy ranges from 58%-69.9% [10]. A few studies which is conducted in Ethiopia also showed that the magnitude of stunting among HIV positive children received antiretroviral therapy in Ethiopia was between 13.4% to 65% [15-17]. The commonest factors for stunting and statically significant includes:- residence, presence of opportunistic infection, frequency of meal, age of the child, income, absence of dietary counseling, late diagnosis of HIV, duration of follow-up at ART clinics, being anemic and the presence of diarrhea were statically significant associated factors with stunting [15-17].
The government of Ethiopia also were adapted different types of strategies and implemented for decreament of the impact of HIV/AIDS on the nutrition status of children including by preparing consolidated comphernsive national ART guidelines for ART care and treatment, and sustainable development goal (SDG) #2 to end hunger, achieve food security and improved nutrition and promote sustainable agriculture yielding marked success in reduction of HIV and stunting patient morbidity and mortality respectively [18,19]. There is also a livelihood support and food assistance, strengthened communitybased nutrition care and support activities of PLWHIV [18,20]. The magnitude of stunting is a serious common public health problem of 51.63% HIV positive children received ART in Ethiopia and the impact of stunting on immune cell level on clinical follow up remains largely unknown [21]. Therefore the aim of this study was to assess stunting as common dependent variable and associated factors of socio-demographic variables, clinical related factors with them further variables.
Study area
The study was conducted at Amhara public hospitals of Debre Markos Comperensive Specialized Hospital, Shegaw Motta General Hospital, and Finot Selam General Hospital Northwest Ethiopia [22-24].
Study design
An institutional –based cross-sectional study.
Study populations
All children HIV-infected patients who received ART and available during the data collection period..
Eligibility criteria
We included childern patients who were age greater than 2 years old and complete file.
Sample size determination and sampling procedure
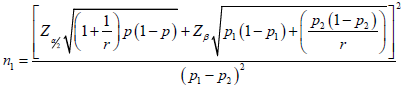
We checked the adequacy of sample size based on the objectives. The sample size was calculated using a difference between two population proportions formula, by considering the following conditions with 5% level of significance (α), at 95% level of confidence for the two-tail test, r is the ratio of the size of sample 2 to sample 1=1 and a Power of (1B)=80%. The required sample size is 372 [25]:-
• Proportion of HIV infected wasted children of male 12.9% and of female 34.9%
• Proportion of HIV infected underweight children of male 24.7% and of female 16.4%
• Proportion of HIV infected stunted children of male 34.3% and of female 26.2%.
• With 5%level of significance (α), at 95% level of confidence for two tail test, r is the ratio of the size of sample 2 to sample 1=1 and a Power of (1-B)=80% (Table 1).
| Undernutrition | r | P1 (Male) | P2 (female) | P (pooled) | Zα/2 | Zβ | n1 | n2 | Ni | FPC N | Nf |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Wasting | 1 | 0.129 | 0.086 | 0.349 | 1.96 | 0.84 | 514 | 514 | 1028 | 581 | 372 |
| Underweight | 1 | 0.247 | 0.164 | 0.5779 | 1.96 | 0.84 | 234 | 234 | 468 | 581 | 168 |
| Stunting | 1 | 0.343 | 0.262 | 0.7533 | 1.96 | 0.84 | 318 | 318 | 636 | 581 | 304 |
 is the common population proportion
is the common population proportion
So the required sample size by taking the largest sample was 372, then we used systematic sampling technique.
Variables
Dependent variable: Stunting (yes/no)
Independent variables: Data were socio-demographic characteristics including age, sex, educational attainment of a mother, orphan hood, Family size, nutritional support and counseling, meal frequency. Dietary and food security-related factors information also included food group of grain, pulse, fruit and vegetables, vitamins, egg, meat, fat and oils, and milk and milk products and clinical related factors includeds- diahrea diseases in the two last weeks, HAART treatment, prophylactic treatment status, Adherence status of ART, OIs, Presence of comorbidity, HIV diagnosis, CD4 count, and stage of WHO.
Operational definitions
• Stunting: Children having height-for-age (HAZ) below -2 SDs of Z-score [5].
• Dietary diversity: The number of reported different foods and food groups consumed in an individual’s over 24-hour. This includes food groups consumed by outside home and less than 4 and greater or equal to 4 food group are fair/poor and good dietary diversity respectively [26].
• Adherence to ART: The recent adherence status of the adult to the ART which is recorded as poor when an adult takes less than 85% of the dose, fair when he/she takes 85-94% of the dose, and good when he/she takes 95% and above of the dose [18].
• Comorbid disease: A chronic disease with a confirmed diagnosis of the disease other than HIV infection [18].
• Opportunistic infections/diseases: The list of opportunistic diseases indicated on national comprehensive HIV prevention, care, and treatment [18].
Data collection and quality control
Data were extracted from compherensive and consolidated ART care and treatment checklist [18], the Food and Agriculture Organization (FAO) standardized verbal questionnaires [27] and prepared from the previous work of literatures [26,28,29]. We used an interviewer-administered and a structured questionnaire to collect the data. The height measurement of children were taken by using the standardized measuring scale. Children ' take off their shoes, stand erect, and look straight in the horizontal plane. The occipital, shoulder, buttocks, and heels touched the measuring board, and height was recorded to the nearest 0.1cm on a standing position. The presence or absence of bilateral pitting pedal edema also was also assessed. Anthropometric measurements were converted to physical growth indicator of (HAZ) and used both WHO anthro and WHO anthroplus software. Three nurses currently working in the ART clinics were recruited involved as data collectors. To maintain data quality, the questionnaire was first developed in English then translated to Amharic and back to English. The tool was pre-tested on 10% of the total sample size at Bichena Health Center. To assure data quality, daily supervision was done by the principal investigator. Two-day training was given for both data collectors and superivor concerning the data collection tool and the data collection process. Moreover, all collected data were checked for completeness and consistency during the data management, storage, and analysis phase by the research team members.
Statically analysis
Data were entered through EPI DATA version 4.1, and analysis was made using STATA version 14.1 statistical packages. Descriptive statistics of categorical variables were visualized using tables and graphs whereas results of continuous variables were described using measure of central tendency (mean and media), and dispersion (standard deviation and range). Bi-variable association between each individual explanatory variable and under nutrition was evaluated using odds ratio (OR) with the corresponding 95% confidence interval (CI) as a parameter estimate. In the next step, we purposely included additional explanatory variables which were statistically significant a p-value of <0.25 to build an empirical model. In our analysis, a potential problem of multicollinearity was checked using variance inflation factor (VIF) at cut off point of 10. Interaction was also checked and we found no significant interaction terms. Finally, in the multivariable binary logistic model, a p-value of <0.05 was considered to declare statistical significance with the corresponding 95% confidence interval. The goodness of fit (GOF) of our model was checked using Hosmer-Lemeshow GOF test. The p-value of the Hosmer-Lemeshow GOF test of this model is p-value greater than 0.05 which confirms that the model is correctly specified.
Socio-economics characteristics of the study participants
A response rate of 100% with most 96(51.6%) children were males and majority 290 (78) of were being urban areas. The mean (± SD) age of children included in the study was 8.8 (± 3.2) years ranging from 2year to 14 years. More than 133 (35.8%) parent were married, and Majority 300 (80.6) of children had mother (Table 2).
| Variables | Frequency (N) | Percent (%) |
|---|---|---|
| Age | ||
| 2-5 years | 54 | 14.5 |
| 5-10 years | 149 | 40.1 |
| 10-15 years | 169 | 45.4 |
| Maternal Marital Status | ||
| Married | 133 | 35.8 |
| Divorced | 74 | 19.8 |
| Windowed | 75 | 20.2 |
| Others* | 15 | 4 |
| Maternal Educational Status | ||
| Can not read and write | 99 | 26.6 |
| can be read and write | 53 | 14.2 |
| 1-8 grade | 58 | 15.6 |
| 9-12 grade | 44 | 11.8 |
| College/university | 43 | 11.6 |
| Family size | ||
| 01-Mar | 189 | 50.8 |
| 04-Jun | 162 | 43.5 |
| >6 | 21 | 5.6 |
| Meal Pattern Per 24 Hours | ||
| Three and above | 227 | 61 |
| Below three | 105 | 28 |
| Do not know | 41 | 11.2 |
| Nutritional Support and Counseling | ||
| Yes | 80 | 21.5 |
| No | 292 | 78.5 |
Dietary diversity-related factors of participants
More than half of 200 (52.3%) children were ate fair/poor food variety per 24 hours. Majority 330(80.64) 335(90%), 312(83.87%), and 295 (79.30%) of children ate food groups of grain, pulse, egg, and meat and meat products respectively (Figure 1).

Figure 1. Individual dietary diversity of characteristics of the study participants at Amhara Regional Public Hospitals, Northwest, Ethiopia, 2018.
Clinical related characteristics of HIV infected children
Two-third 251(67.5%) of children were have taken HAART regimen of (ABC + 3TC + LPV/r) and one-tenth 41(11%) of where have taken 2e (AZT + 3TC + LPV/r). Most 369(99%) of children were diagnosed a virus in the blood greater than 12 months and more than two-third 284 (78.3%) of children had no diarrhea in the last 2 weeks. Most 343(92.2%) of were received ART greater than 12 months and 301(89.9%) and 340 (91.4%) were an early stage of WHO (I&II). Majority 84.6% and 79.2% of children had CD4 ≥ 500cell/mm3 in the current and in the last 6 months respectively. Majority 299(80.4%) of children did not develop comorbidity diseases (Table 3).
| Variables | Frequency (N) | Percent (%) |
|---|---|---|
| Virus occurred in the blood | ||
| ≤12 months | 3 | 0.8 |
| >12 months | 369 | 99.2 |
| OI | ||
| Yes | 177 | 47.6 |
| No | 195 | 52.4 |
| Stage of WHO | ||
| Ealy stage(I&II) | 301 | 80.9 |
| Advanced stage (III&IV) | 71 | 19.1 |
| Prophylactic therapy | ||
| Yes | 292 | 78.5 |
| No | 80 | 21.5 |
| ART duration | ||
| ≤12 months | 29 | 7.8 |
| >12 months | 343 | 92.2 |
| Comorbidity diseases | ||
| Yes | 73 | 19.6 |
| No | 299 | 80.4 |
| ART adherence | ||
| Good | 310 | 83.3 |
| Fair/poor | 62 | 16.7 |
| HAART regimens | ||
| AZT + 3TC + LPV/r | 41 | 11 |
| ABC + 3TC + LPV/r | 251 | 67.5 |
| ABC + 3TC + EFV | 71 | 19.1 |
| TDF+3TC+EFV | 9 | 2.4 |
Magnitude of stunting among HIV positive children
The magnitude of stunting was found to be 45.2%, 95% CI (40.4-50.0).
Associated factors of stunting among HIV positive children
Variables with (P-valve <0.25) of residence, age of a child, educational status of mother, marital status, family size, dietary diversity, CD4 cell count, duration of ART, co-morbidity disease, OI, and diarrhea were associated factors with stunting in binary bivariable logistic regression analysis. Only three variables were identified as statically significant associated factors of stunting. Accordingly being male children were male 1.94 (AOR=1.942, 95% CI: 1.188, 3.175) times more likely developed stunting as compared to females. Children who were age group b/n 2-5 years old were 58% times more likely to develop stunting as compared to the age group 10-15 years old (AOR:0.434,95% CI: 0.253,0.746). Participants who had opportunistic infections 2.41 (AOR: 2.41, 95%, CI: 1.61, 7.60) times more likely to develop stunting as compared to the counterpart. Moreover, children who had fair/poor individual dietary diversity were 1.83(AOR=1.832, 95% CI (1.128.2.95) times more likely to develop stunting as compared to children who had good dietary diversity (Table 4).
| Variables | Stunting | COR95%CI | AOR95%CI | p-value | |
|---|---|---|---|---|---|
| Yes | No | ||||
| Sex of the Child | |||||
| Male | 96(51.6) | 90(48.2) | 1.689(1.119,2.550) | 1.942(1.188, 3.175) | 0.002 |
| Female | 72(38.7%) | 114(61.3) | 1 | 1 | |
| Age of Child | |||||
| 2-5 year | 33(61.1%) | 21(38.9%) | 1 | 1 | |
| 5-10 year | 47(31.5%) | 102(68.5%) | 1.446(0.77,2.702) | 0.223(0.161,3.206) | 0.143 |
| 10-15 year | 88(52.1%) | 81(47.9%) | 0.424(0.268,0.671) | 0.434(0.253,0.746) | 0.04 |
| OI | |||||
| Yes | 109(61.6%) | 68(58.4%) | 1.12(1.34,1.98) | 2.41 (1.61, 7.60) | 0.018 |
| No | 115(59%) | 80(41%) | 1 | 1 | |
| Dietary Diversity | |||||
| Good | 80(45.5%) | 96(54.5%) | 1 | 1 | |
| Fair/poor | 108(55.1%) | 88(44.9%) | 1.023(0.679, 1.539) | 1.832(1.128, 2.95) | 0.001 |
In this study, 45.2% (95% CI: 40.4-50.0) children were stunted which is aligns with studies, which is condacted at East Africa 48.21% -51.63% [21]. However, this finding lower than the report of some studies which is conducted in Ethiopia 65% [15], and India 69.8% [30]. Conversely, this study finding is much higher than the study reported in Adama, Ethiopia stunting about 13.4% [16], 30% in eastern Ethiopia [17], and 27% in Nigeria [31]. The above variation could be explained by the difference of sample size, study setting, feeding habits, culture, economic status, a sample size of care providers/parents, ART duration, and socio-demographic characteristics of study participants.
This study depicts that being male, age group of 2-5 years, presence of OI, and fair/poor dietary diversity were significant factors with stunting. In this study being male was a statically significant factor with stunting. This finding is consistent with studies which are reported in Ethiopia [16], and Tanzania [31]. This finding contradicts also findings from a study reported from India [32], and Gonder, Ethiopia [15]. The varation could be explained due to difference of cultural feeding practice and sample size. The association between gender and malnutrition remain unclear and need further investigation [33], but in this study, the variation was due to most of male child-mother occupation were daily workers and lack of awareness of the use of diversified diet.
This study also revealed that being age group of 2-5 years old was a statically significant factor with stunting. Children who were being the age group of 2-5 years old were more likely developed stunted as compared to the age group of 10-15 years. This find aligns with the studies which are conducted in Ethiopia [15]. The possible explanations for these findings were age group of 2-5 years/ younger children were weaning from the breast, inadequate supplementary feeding, loss of passive immunity, and more leading to recurrent infections and a poorly nourished child at this age. Additionally, opportunistic infections were statistically significant associated factors with stunting. These findings are consistent with the studies which are conducted in Adama, Ethiopia [16], and Nepal [34]. The possible explanation might be an opportunistic infection that affects the nutritional status of the child which leads to undernourished through distortion of food intake, abosbation, and increased utilization and excretion of nutrients and fasten the progression of the disease [12].
Finally, this study found that children who had fair/poor, dietary diversity were statically significant associated factors with stunting. This finding is consistent with studies conducted in Hawassa, Ethiopia [25]. The possible reason might be that a patient did not get variety of food that that have enhanced for different types of infection and compromised the immunity of the patient that developed stunting [35].
In the present study, more than two-fifth of the study children was developed stunting among HIV-positive children. Age of children 2-5 years, being male, presence of opportunistic infections and fair/poor individual dietary diversity increased the risk of stunting among children living with HIV. Therefore policymakers and clinicians should be a focus, early detection of opportunistic infections, control progression of HIV, educating and counseling the use of the diversified diet, monitoring this situation is highly recommended.
The study has several limitations. It cannot show a cause-effect relationship between the variables since the study design was hospital cross-sectional. There may be measurement bias and recall bias for individual dietary diversity and it might also undermine the generalization of the study result to the general population.
Ethics approval and consent to participants
The study was given ethical clearance [Protocol Identification Number: MS-Et/M.3-P 4.4/2015-2016] by the Ethical and Protocol Review Committee of the College of Health Sciences, University of Ghana. Permission was obtained from the clinician-in-charge of the HIV clinic at the KBTH and informed consent was sought and obtained from each study participant. Patients' data were deidentified during data capture, entry, analysis and storage by ensuring only the study codes were used consistently throughout the project cycle.
Not applicable.
YS: Conception of a research protocol, literature review, study design, data analysis, interpretation, and drafting of the manuscript. YS, NAM, AEG, BTZ, and MG: Data analysis, interpretation, and manuscript review. All authors have read and approved the manuscript.
We acknowledged all selected study site officials who allowed us to conduct this project on their clients. Likewise, we are thankful to all data collectors and respondents for their willingness for the interview.
Journal of AIDS & Clinical Research received 5264 citations as per Google Scholar report



