Research Article - (2022) Volume 13, Issue 1
Received: 08-Dec-2021, Manuscript No. jfr-21-49227;
Editor assigned: 09-Dec-2021, Pre QC No. P-49227;
Reviewed: 15-Jan-2022, QC No. Q-49227;
Revised: 22-Jan-2022, Manuscript No. R-49227;
Published:
28-Jan-2022
Citation: Fugiwara, FlÃ?via Vanessa Greb, Deisy Satie Moritsugui, FlÃ?via Nicolle Stefani Vassallo and Rassa Ananda Paim Strapasson, et al. Assessment of the Accuracy of Facial Linear Measurements on Horos Software. J Forensic Res 13 (2022): 483.
Copyright: © 2022 Fugiwara FVG, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Objectives: This study verified the reliability and accuracy of linear measurements performed in CBCT in Multi Planar Reconstruction (MPR), in MIP visualization mode, at minimum (STmin) and maximum (STmax) slab thicknesses for quantitative evaluation of facial anatomical structures.
Materials and methods: 17 skulls from biobank of the Laboratory of Forensic Anthropology and Dentistry of University of São Paulo (OFLab- FOUSP) were selected for measurement of 10 linear distances. The skulls were measured in three different ways, one directly on the skull (gold standard) and two on Horos Software (in STmin and STmax). Direct measurement on skull was compared to indirect measurements. Thus, group A (skull-STmin) and group B (skull-STmax) were analysed and the significance level of 5% was adopted.
Results: Inter- and intra-examiner ICC (Intraclass Correlation Coefficient) was excellent. The consistency of measurements between the methods in groups A and B was verified by Bland-Altman analysis. Group B showed greater measurement accuracy, however, mean difference was found smaller than 1 mm in group A.
Conclusions: Craniometric measurements performed at any thickness interval between the minimum and the maximum can be considered reliable for craniofacial anthropometric analysis, apart from measurements located in the midline of the skull base.
Forensic anthropology • Craniofacial analysis • Craniofacial anthropometry • Dynamic features • Radiology
Craniofacial anthropometry is a method of quantitative assessment of facial anatomical structures [1] used to predict the facial profile, supporting information that [2] can help in identification of forensic and archaeological cases. Anthropometric evaluation can be performed directly on the skull or indirectly, through images [1]. There has been a substantial increase in open source softwares seeking to develop competitive image managing tools, especially regarding to post-processing [3].
The evolution of craniofacial imaging, in particular with the use of cone beam computed tomography (CBCT), has contributed to refine the knowledge on anatomical structures [4]. In the field of Forensic Dentistry, it is possible to use this imaging exam for age estimation [5], anthropological and morphological analysis of the skull [6-8], as well as evaluating facial soft tissue thicknesses for forensic facial approximation [7-10]. CBCT is quite reliable for linear measurements [11] but the precision and reliability of the program used should be considered just as much.
The way the image is visualized can interfere with the results of the measurements. Software that allow the visualization of images in DICOM format were developed and tested concerning the accuracy and precision of the measurements performed with these tools [4,11–23]. It is possible to reconstruct the volume acquired in CBCT exams in multiplanar reconstruction (MPR), a technique that allows the analysis of images obtained in axial plane, in the sagittal and coronal planes. Thereby, the slabs can be individually evaluated in the three planes and in different thicknesses. Another important visualization tool, MIP (Maximum Intensity Projection), selects and highlights the voxels with maximum brightness, that is, it detects structures with high contrast, hence, it is used preferably to display mineralized structures [22].
The aim of this study was to assess the reliability and accuracy of linear measurements performed in CBCT in MPR, in the MIP visualization mode, in the minimum and maximum slab thicknesses (STmin and STmax, respectively) for application in both Forensic Imaging and in the daily clinical routine (Figures 1A and 1B).

Figure 1A. MIP visualization, STmin in sagital, axial e coronal planes.

Figure 1B. MIP visualization, e STmax in sagital, axial e coronal planes.
This study was approved by the Ethics Research Committee of the Faculty of Dentistry of University of São Paulo under report number 4.631.887. Seventeen skulls belonging to biobank of the Laboratory of Anthropology and Forensic Dentistry of the University of São Paulo (OFLab-FOUSP) were selected for the measurement of 10 linear lengths, measured in three different ways: one directly on the anatomical structure of the skull, used as reference for comparison to other measurements (gold standard) and two other approaches indirectly, through images. The craniometric landmarks and the measured linear lengths are specified in Tables 1 and 2, respectively.
| Craniometric Landmarks | Definitions |
|---|---|
| Opisthocranion (op) | Most posterior midpoint on the occipital bone, usually above the outer occipital protuberance. |
| Euryon (eu) | Most lateral point of the cranial vault, on the parietal bone. |
| Basion (ba) | Point in the median plane on the most anterior portion of the anterior edge of the foramen magnum. |
| Zygion (zy) | Most lateral point on the zygomatic arch. |
| Zygomaxillare (zm) | Inferior point on the zygomaticmaxillary suture. |
| Ectoconchion (ec) | Lateral point on the orbit on the line that bisects the orbit transversely. |
| Nasion (n) | Intersection of nasofrontal sutures in the median plane. |
| Glabella (g) | Median point more projected anteriorly on the frontal bone, between the supraciliary arches. |
| Linear distances | Abbreviation | Craniometric Landmarks | Slab in HorosTM | |
|---|---|---|---|---|
| Maximum skull length | MSL | op-g | Sagital | |
| Maximum skull width | MSW | eu-eu | Axial and coronal | |
| Skull base length | SBL | ba-n | Sagital | |
| Maximum facial width | MFW | zy-zy | Axial and coronal | |
| Medium facial width | FW | zm-zm | Axial and coronal | |
| Bi-orbital width | BOW | ec-ec | Coronal | |
| Orbit height | OH | NA | Coronal | |
| Nose width | NW | NA | Coronal | |
| Nose height | NH | n-ns | Coronal and sagital | |
| Anterior mandibular width | AMW | ml-ml | Axial and coronal | |
Direct measurement
Direct measurements on the skull were performed with a digital caliper (Mitutoyo®, Mitutoyo Sul Americana, Suzano, Brazil) and Bertillon's Compass and were considered the gold standard for data analysis.
Indirect measurements
Indirect measurements were performed on cone beam computed tomography (CBCT) which were obtained on an i-CAT tomograph (Imaging Sciences International, Hatfield, Pennsylvania, USA), FOV 23 × 17 cm, 0.4 mm voxel, 120 kVp, 36.12 mAs and 40 sec exposure time, and a dry skull positioner for extra-oral radiographic examinations, which kept them in a stable and standardized position [24].
The DICOM files were imported to HorosTM Software v 3.3.6 – 64 bits (Horos Project, Purview, Annapolis, USA), and measurements were performed as follows: image reconstruction was selected in MPR and WL (Window Level) was fixed at 500 and WW (Window Width) at 3500, the image visualization mode chosen was MIP (FIG. 1A and 1B) and the skull images were oriented in such a way the Frankfurt plane was parallel to the horizontal plane. Thereby, measurements of linear lengths were first obtained in STmin (Figure 2A); and, in the second approach, in STmax (Figure 2B).

Figure 2A. Measurement in STmin .

Figure 2B. Measurement in STmax.
Statistical analysis
Jamovi software (Jamovi Project, 2021, Version 1.8- Computer Software Open Access) was used for statistical analysis. The significance level adopted for the analysis was 5%. The intra-observer correlation of the 3 researchers, and inter-observer correlation between the two researchers who performed the indirect measurements, both in STmin and STmax thickness, were verified by the Intraclass Correlation Coefficient (ICC). The values of linear measurements obtained were inserted into an Excel sheet (Microsoft Excel for Mac, version 16.48, Redmond, WA) and compared to real values obtained directly on the skull and Stmin (Group A) and real values obtained directly on the skull and STmax (Group B). For each of the referred groups, the consistency of the methods was verified using the Bland-Altman analysis.
The intra-examiner Intra-Class Correlation Coefficient of the three researchers was higher than 95% in all methods (Table 3). The inter-examiner concordance (Table 4) among the researchers who executed the digital measurements showed good agreement in both methods, STmin and STmax, of 80%.
| Estimated Correlation | |||
|---|---|---|---|
| 95% Confidence Interval | |||
| Concordance | Lower | Upper | |
| Gold standard examiner | 0.999 | 0.998 | 1 |
| Researcher 2 STmin | 0.999 | 0.998 | 0.999 |
| Researcher 2 STmax | 0.997 | 0.995 | 0.998 |
| Researcher 3 STmin | 1 | 0.999 | 1 |
| Researcher 3 STmax | 0.994 | 0.989 | 0.997 |
| Estimated Correlation | |||
|---|---|---|---|
| 95% Confidence Interval | |||
| Concordance | Lower | Upper | |
| STmin | 0.812 | 0.694 | 0.888 |
| STmax | 0.807 | 0.685 | 0.884 |
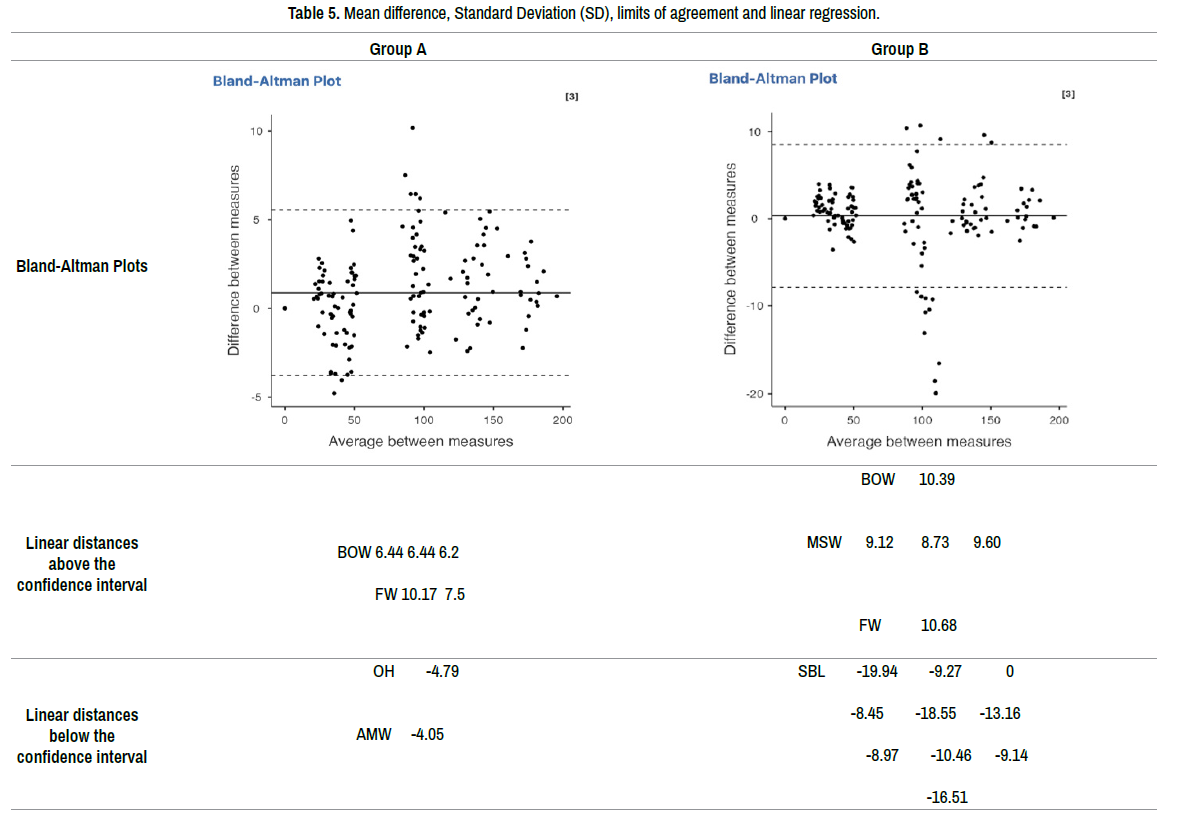
Table 5 indicates, for each group, the mean difference between the compared methods, standard deviations, and upper and lower limits of the confidence interval (95%). The result of the linear regression test presented p-value higher than 0.05 only in group B, which, therefore, did not show proportion bias between measurements.
The analysis of accuracy and reproducibility of CBCT craniometric measurements using public domain software can represent, in some circumstances, an improvement in interoperability, facilitating the exchange of data between different programs, allowing a faster and more effective data sharing. The free access to its tools makes software, such as HorosTM, important allies of health professionals and students, who seek to improve their abilities on handling its functionalities, facilitating workshops and enabling effective clinical training [3].
Post-processing image quality is important for quantitative analysis of maxillofacial hard tissue [19], considering that it depends on the software's capacity to reconstruct the image from the 3D volumetric data set acquired in CBCT. However, the choice of the technique for 3D image volume reconstruction in CBCT is attributed to the operator, who determines the best way to reconstruct CT slabs depending on the purpose of the study and their preferences [26,27].
Many factors can affect the operator's visual perception in linear measurements such as image contrast, image noise, individual visual perception and prior knowledge of anatomy [28]. The WL and WW values refer to the contrast he image to be analyzed [29], so different windowing values influence visualization of bone limits, being more or less evident depending on the width (W) and level (L). In this study, the defined WL and WW values allowed an adequate perception of the bone margins and structures for measurement.
Visualization and location of craniometric landmarks on curved surfaces is difficult on rendered 3D image [28]. Nonetheless, the MPR allows the operator to visualize the craniometric landmark, on the selected slab, on the three viewing windows, simultaneously [30]. The use of MPR is indicated for quantitative assessments, as the measurements would highly correspond to real anatomical structures [20-22] and would be more accurate than the rendered view mode, which in this case is more suitable for a qualitative assessment [14-28].
The selection of the slab, in the axial, coronal and sagittal planes, requires time, calibration training [31] and careful evaluation by the examiner [23]. The precise location of the craniometric landmarks is crucial for linear measurements [4], since, in MPR, the operator goes through the three windows to identify them [17]. However, the selection of the starting and ending point for measurement must be performed in a single plan. In this study, it was observed a high level of ICC, both intra and inter-examiners, which as due to the training and alignment of the researchers, prior to the measurements. These results corroborate previous studies, which demonstrated excellent reproducibility and consistency in measurements in MPR [23-31].
The analysis of measurements in group A (skull-STmin), in the Bland Altman analysis, demonstrates a tendency of measurements performed directly on the skull to be overestimated in relation to measurements in STmin, revealing five measurements above the upper limit (5.530) of the interval confidence. Three of these measurements are related to the bi-orbital width (BOW), determined by craniometric points (ek-ek) located in tunnel-shaped anatomical structures, in this case, the orbits. Such characteristic, already considered in a previous study [21] may overestimate the diameter measured with the caliper. The other two measurements are related to the mean facial width (FW), determined by the zm-zm distance, where zm was often not clearly visualized due to calcification of the zygomatic-maxillary suture.
The measurements considered on group B (skull-STmax) presented five measurements above the upper limit (8.485) of the interval confidence. Three measurements were related to the maximum skull width (MSW), in which the values of the distance between eu-eu obtained by the gold standard were higher than the ones in STmax. This effect may have occurred due to the variability on the perception of the localization of the point by the observers. Ten measurements related to ba-n distance, equivalent to the skull base length (SBL) were below the lower limit (-7.841) of the interval confidence, demonstrating that the reference measurements tend to be lower than the STmax measurements. This result conflicts with other studies which demonstrated that the measurements in MPR were smaller than the real distances, significantly at the base of the skull, in its internal portion [18], which was also observed in 3D rendering [15].
The linear regression test shows that there is a proportion bias in group A (skull-STmin), as p<0.05. The values of the differences between the measurements tended to be heterogeneously distributed, even within the 95% interval confidence, which represents lower agreement between the direct measurement and the measurement in STmin. Analyzing the pattern of the groups in relation to the mean differences, group B (skull-STmax) showed greater agreement in this group, with the exception of the MSW. However, group A showed a lower concordance when compared to group B, with a tendency to higher values in direct measurements. The slab thickness in the MIP visualization mode affects, quantitatively, the appearance of the reconstructed image in CBCT [26,29]. Nonetheless, despite the veracity of this information had been verified in this study, the difference found between the direct and Stmin measurements, p <0.01, in practice, was less than 1 mm, which would not compromise the craniometric analysis.
Considering the findings of this study, the slab thickness selection tool proved to be an important image visualization resource for the specific assessment of cranial anatomical features. The reliability of the technique indicates that its use in craniofacial anthropometric analysis can contribute to identification of human remains, as well as being useful in the reconstruction of skulls that present pathological fractures or those caused by taphonomic factors.
The evaluation of HorosTM software for linear measurements on skulls showed that at higher thicknesses the measurements would be more accurate than at smaller thicknesses. In addition, craniometric measurements performed at any thickness interval between the minimum and the maximum can be considered reliable for craniofacial anthropometric analysis, except for the anatomical structures, when image is reconstructed in MPR, because they may be superimposed in STmax.
The choice of slab thickness selected in MIP depends on the linear length that is wanted to measure. In this study, the linear measurements performed, in MPR and visualization mode in MIP, proved to be reliable when measured in both minimum and maximum thickness, apart from measurements located in the midline of the skull base.
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Cross Ref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Google Scholar Crossref PubMed
Journal of Forensic Research received 2328 citations as per Google Scholar report