Commentary - (2020) Volume 4, Issue 1
Received: 28-Feb-2020
Published:
20-Mar-2020
, DOI: 10.37421/vcrh.2020.4.110
Citation: Wickramasinghe NC, Steele EJ,
Gorczynski RM, Temple R, Tokoro G et al. "Growing Evidence against
Global Infection-Driven by Person-to-Person Transfer of COVID-19." Virol Curr Res 4 (2020) doi: 10.37421/Virol Curr Res.2020.4.110
Copyright: © 2020 Wickramasinghe NC, et al. This is an open-access article distributed under the terms of the creative commons attribution license which permits
unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Examining a sample of still unfolding epidemiological data relating to the world-wide epidemic of Covid-19, we conclude that a connection with an atmospheric in fall appears increasingly probable.
Coronavirus • Epidemiology • Panspermia
Events that are unfolding in relation to the COVID-19 outbreak appear to question the validity of many of our normal assumptions that relate to airborne infectious diseases, epidemics and pandemics Figure 1.
Figure 1: Thinking straight is hard if one is anchored on a shore of ignorance– (Painting by Gerart DuBois)
“A pathogenic virus must always pass from one infected animal (or carrier) to another animal in a causal chain in order to cause an epidemic disease”.
This is a sacred dogma of medical science that has been firmly held and rigorously defended for decades. In the normal conduct of science and philosophy it takes only one decisive contradiction to disprove and dislodge a reigning dogma or theory. We have already argued in an earlier communication that the standard theory is hard pressed to account for many of the emerging facts [1].
In the past several weeks new cases of coronavirus (COVID-19) seem to have appeared in their thousands in a region of China (Wuhan) and then spread within China as well as sporadically to distant locations in the world. The question still baffling everyone is how did it all start and who was case zero [2]?
A summary (necessarily incomplete) of the reported case numbers/statistics as on 27 February 2020 in many countries are as follows:
• China: 78,514 cases; 2,744 deaths
• Asia and Oceania: 3,020 cases; 25 deaths (Philippines, Hong Kong (2), Japan (4), Taiwan, Diamond Princess (4), South Korea (13), India (3), Pakistan (2), Sri Lanka (1))
• Europe: 810 cases; 19 deaths (France (2), Italy (17))
• Middle East: 358 cases; 26 deaths (Iran)
• Africa: 2 cases
• South America: 1 case
• North America: United States (60 cases), Canada (13 cases)
Whilst the escalation in the number of COVID-19 cases globally is a reason for legitimate public health concern, it is prudent to keep in mind the fact that this disease has a lower rate of morbidity (death rate) than seasonal influenza, which is about 2 percent globally. The average death rate from COVID-19 has a similar value in Wuhan, but it is much lower, about 0.7% globally outside China. It also wise to keep our concerns in perspective by noting that this is generally a mild and self-limiting disease and that serious complications are confined to older people with underlying health problems.
The presumption is that the spread occurs only by direct contact with an infected person. That this may not be the entire story has become increasingly apparent when links between individual cases and geographical foci of infection are often difficult to establish. Over a wide region of China around the “epicentre” in Wuhan large numbers of positive detections of COVID-19 were reported throughout November and December 2019 and January and February 2020. We have already highlighted the fact that the several isolates of the virus distantly placed in time and space appear to have little or no genetic variations, implying a “pure culture” of the virus of external origin being maintained over several weeks [2-4]. This situation is difficult to reconcile with a brisk replication of the virus in hundreds of thousands of individuals who are infecting one another - as the viruses will often mutate in transit, however slightly. In this section, we highlight a few instances of the disease (positive COVID-19) that have been brought to our notice where no connection to another infected individual can be traced. It is thus predicted that when sequencing of the RNA genomes of the COVID-19 isolates is performed (from these widely distributed global samples) the sequences will show little or no variation, thus indicative of a common source.
France
The day after the announcement of the death of the first French coronavirus case on February 26th 2020 investigations were conducted to determine the “conditions of contamination” in the Paris hospital of Pitié-Salpêtrière to which the patient was admitted as an emergency. The victim, a 60-year-old teacher, came from Oise. A second patient, also from Oise, was a 55-year-old civilian working on the Creil air base. He was in a serious condition when he was admitted to the intensive care unit at the University Hospital Centre (CHU) of Amiens. According to the sources neither of these two victims had visited China or northern Italy which had become the main epidemic centre in Europe [3].
According to the Director of the Hauts-de-France regional health agency Etienne Champion:
"The two patients from the Oise did not go to high-risk exposure areas. And that is why, at first, they were not identified as possible cases of coronavirus. Investigations are underway to determine the source of the two infections…" (Reported on February 26, 2020).
United States of America
A case of COVID-19 has been confirmed in a Northern California resident in Solano County, (northeast of San Francisco) who had no travel history to an affected area and no known contact with any person previously diagnosed with COVID-19, the Centers for Disease Control and Prevention (CDC) announced today (February 26, 2020).
"At this time, the patient’s exposure is unknown. It's possible this could be an instance of community spread of COVID-19, which would be the first time this has happened in the United States," the CDC said in a statement. "Community spread means spread of an illness for which the source of infection is unknown. It's also possible, however, that the patient may have been exposed to a returned traveler who was infected."
Our comment is that “Community spread” is the trope of ignorance being widely deployed by health authorities the world over. Like “ punctuated equilibrium ” in biology it describes a phenomenon without attempting to understand it in any way.
Japan
Headline: None of Japan's new coronavirus patients had direct China links [4].
• February 13th, 2020: “A Kanagawa Prefecture woman in her 80s died from the coronavirus. Her son-in-law also tested positive for the disease. A doctor in Wakayama Prefecture and a man in Chiba Prefecture are confirmed to have the virus. None of them travelled to China recently or had contact with people who visited Hubei Province, the epicentre of the outbreak. ….. The 80 year old woman's symptoms began Jan. 22 when she felt fatigue, the health ministry said. Symptoms worsened on Jan. 25, prompting her to see a doctor three days later. She was placed under observation. …. The victim was hospitalized Feb. 1, diagnosed with pneumonia. She underwent screening for the coronavirus Wednesday. The test results came back positive Thursday, the day she died. Her son-in-law also tested positive for the coronavirus. The man, a taxi driver in his 70s living in Tokyo, has been hospitalized since February 6, but the symptoms are reportedly mild. He developed a fever Jan 29.
• “A doctor in Wakayama Prefecture south of Osaka has been infected with the virus, prefectural officials said Thursday. The man, in his 50s, has been hospitalized with symptoms of pneumonia, but is otherwise in stable condition. The doctor did not travel outside the country in the 14 days prior to the onset of symptoms, nor can any contact with people coming from China be confirmed. Wakayama officials suspect the infection had domestic origins.”
• “Elsewhere, a man in his 20s from Chiba Prefecture near Tokyo is also confirmed to have the virus. He developed a fever and other symptoms February. 2. The man reportedly has neither travelled overseas nor had contact with other infected individuals. ”
• “Besides the outbreak on the Diamond Princess cruise ship, which has infected over 200 people aboard the vessel quarantined in Yokohama, 29 cases of coronavirus had been confirmed inside Japan through Wednesday. ”
• “These cases raise new challenges for health officials, who until now had been trying to contain the virus by closely monitoring people with the possibility of contracting the disease. If more people with no direct links to China become sick, determining infection routes will become impossible.”
Source: Yusuke Kurabe, Nikkei staff writer, in Nikkei Asian Review
February 13 13, 2020 22:37 JST Updated on February 14, 2020 04:52 JST
Italy
In the Italian outbreak of CORONA2019 the search for the first patient goes on with little success:
"…As for the alleged ‘zero patient’ the manager returning from China, it turned out that he had not had the coronavirus. From tests carried out on the friend of the 38-year-old Codogno (patient 1) who had been to dinner with him after having returned from China, "it emerged that he did not develop antibodies," explained Deputy Health Minister Pierpaolo Sileri in the evening. "The man had already tested negative for the first coronavirus test. Therefore, he did not start spreading the virus in the Lodi area [5]."
United Kingdom
A man from Surrey has been taken to a hospital isolation unit after becoming the UK’s 20th confirmed case of coronavirus.
He is allegedly the first patient in England to catch the illness in the UK. It appears to be unclear whether he contracted it directly or indirectly from someone who had recently returned from abroad…..
“This is being investigated and contact tracing has begun……”
From Guardian 29 February 2020 [6].
As we keep searching for case zero in many instances where a sudden development of COVID-19 clusters are seen, the global distribution of cases as it unfolds is worthy of comment. As of 29 February the situation world-wide is displayed in Figure 2.
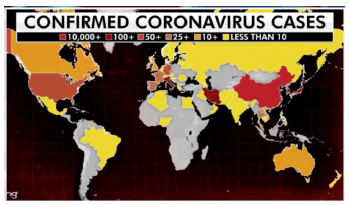
Figure 2: The distribution of COVID-19 cases as on 29 February 2020 [7].
The distribution of cases can be accommodated within a stratospheric deposition model of the kind first discussed by Hoyle and Wickramasinghe [8]. It is of interest to note that the early disposition of cases reported in the USA is uncannily similar to the distribution of cases recorded in case of the H3N2 (Hong Kong flu) pandemic which started in 1968 [9]. In Figure 3a we compare the current picture of COVID-19 in the USA with the progress of the spread of the 1968 Hong Kong flu pandemic. The development of cases from weeks 40-45 (top two frames) is beginning to look uncannily similar to the early phases of the COVID-19 epidemic as it is first making its tentative entry into the United States. Whether later spread of COVID-19 follows the trend shown in Figure 3b is left to be seen.
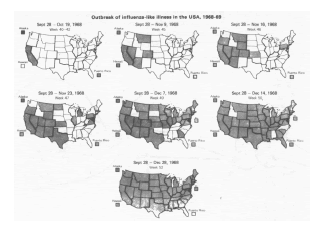
Figure 3a: The spread of influenza H3N2 in 1968 in the USA [8,9].
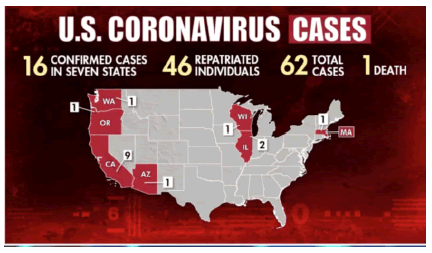
Figure 3b: The distribution of COVID-19 cases as on 29 February 2020 [7].
A fast changing scene
The data that we have discussed in this communication is necessarily in a state of rapid flux, and eventually it may become more difficult to disentangle competing processes and the modes of spread of the disease. As of 29 February 2020 it seems fairly clear that a primary infall process that is both geographically and temporally patchy is followed by varying degrees of efficacy of person-to-person spread. It is tempting to speculate that the latter could be contingent on the variations in habits of greeting around the world – eg Namaste (hands together) in the Indian subcontinent, embrace and hugging through the middle East, and the predominantly western handshake.
Note added in proofs
The proposal to rename COVID-19 to SARS-CoV-2 could fortuitously fit in with our arguments for a putative space origin of both SARS-CoV-1 and SARS-CoV-2. Wickramasinghe et al. [10] had already argued that the 2003 SARS outbreak first appearing in China may have been linked to the dispersal of viruses into the stratosphere from a cometary bolide. We note that the first cases of SARS-CoV-1 recorded in November 2002 appeared a few weeks after a bright cometary bolide exploded in the Ikutsk region of Siberia [11]. It was suggested that the SARS-virus-dust could have been deposited in the stratosphere and subsequently carried by Westerlies to fall first over China. The events of 2002 bear an uncanny similarity to the events that followed the sighting of the Jilin fireball in October 2019 [1].
The case against person-to-person transmission as the sole mode of transmission of the new virus is beginning to grow by the day. Whenever a long-held belief system fails to account for emerging new facts humans have had a long history of turning away from facts or even resorting to deception and falsehood. Let’s hope this will not happen in the present case! Should we not honestly declare that we simply do not know?
We are grateful to Drs. R. Equem and M. Vitaly for alerting us to news about France and Italy.
Virology: Current Research received 187 citations as per Google Scholar report



