Opinion - (2021) Volume 9, Issue 2
Received: 03-Mar-2021
Published:
25-Mar-2021
, DOI: 10.37421/2472-128X.2021.9.172
Citation: Laura, Angelina. Cancer Genomic Drug Therapy. J Clin Med Genomics 9 (2021) doi: 10.37421/jcmg.2021.9.172
Copyright: © 2021 Laura A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
From the past 2 eras, we have gone from a period where most of the new agents were relatively nonspecific chemotherapeutics to an era defined by therapies which are targeted against the specific molecular targets, primarily growth factor receptors or related kinases. These new agents altered our ability to treat the patients across a broad range of diseases and thoroughly transformed to the treatment of few specific cancers. Regarding targeted molecular therapeutics information grew, and the number of new agents has increased, and it became obvious that biology imposed real limits on the success of targeted therapeutics, a realization which led to the other shift in cancer therapy. When it is targeted therapeutics continue to be developed, and signal successes still occur, they no longer represent the sole or even preeminent approach to new cancer treatment [1].
In late 90s, the emerging biologic understanding of human cancer led to the development of the numerous targeted therapies. Early successes include agents like imatinib for chronic myeloid leukemia (CML) and trastuzumab for HER2-positive breast cancer and followed a novel and powerful approach to the cancer problem. The basic evidence of this approach is involved in identifying a molecular lesion or its molecular pathway, measuring its activity in the clinic, and developing an appropriate drug to inhibit function. Various targeted agents took advantage of the oncogenic addiction pathways of cancer cells. One additional assumption underlying this approach was that molecularly targeted therapies would not only prove to be more effective than classic chemotherapeutics, but would also be associated with reduced toxicity, a function of their exquisite molecular sensitivity [2].
Perhaps it is known as the best agent to use this approach was the TKI (Tyrosine Kinase Inhibitor) imatinib for CML (Chronic Myeloid Leukemia). Chronic myeloid leukemia, a myeloproliferative neoplasm characterized by the dysregulated production and proliferation of mature granulocytes, is associated with the fusion of the BCR gene (on chromosome 22) with the ABL1 gene (on chromosome 9), resulting in the BCR-ABL1 fusion gene. This fusion gene has a unique product and abnormal, the BCR-ABL1 fusion protein, which is constitutively active and implicates the pathogenesis of CML. The discovery of imatinib, an oral TKI that competitively binds to the BCR-ABL fusion protein and inhibits its activity, revolutionized the way in which we understood and treated CML. Even prior to a high successful phase III trial,1 the first CML-focused trial clearly established imatinib as a world beater and game changer, replacing a much more toxic and less accessible transplant-based approach.
It is relatively too trivial sequence whole-cancer genomes; this is allowing the scientists to evaluate the relativity of burden and distribution of mutations across tumour types. Besides all these genome-wide sequencing is now readily accessible, identification of genes that drive tumour formation versus so-called “passenger genes” has become a major challenge. Cancers defined by genomic chaos include those driven by exogenous carcinogens, such as a large proportion of malignant melanoma, NSCLC, and HNSCCs (Head and Neck Squamous Cell Cancers). The higher mutational burden of tobaccoinduced HNSCC is comparable to that of other smoking-related malignancies like lung adenocarcinoma and small cell lung cancer [3]. Moreover, the genetic intratumoral heterogeneity can contribute to the treatment failure and drug resistance.
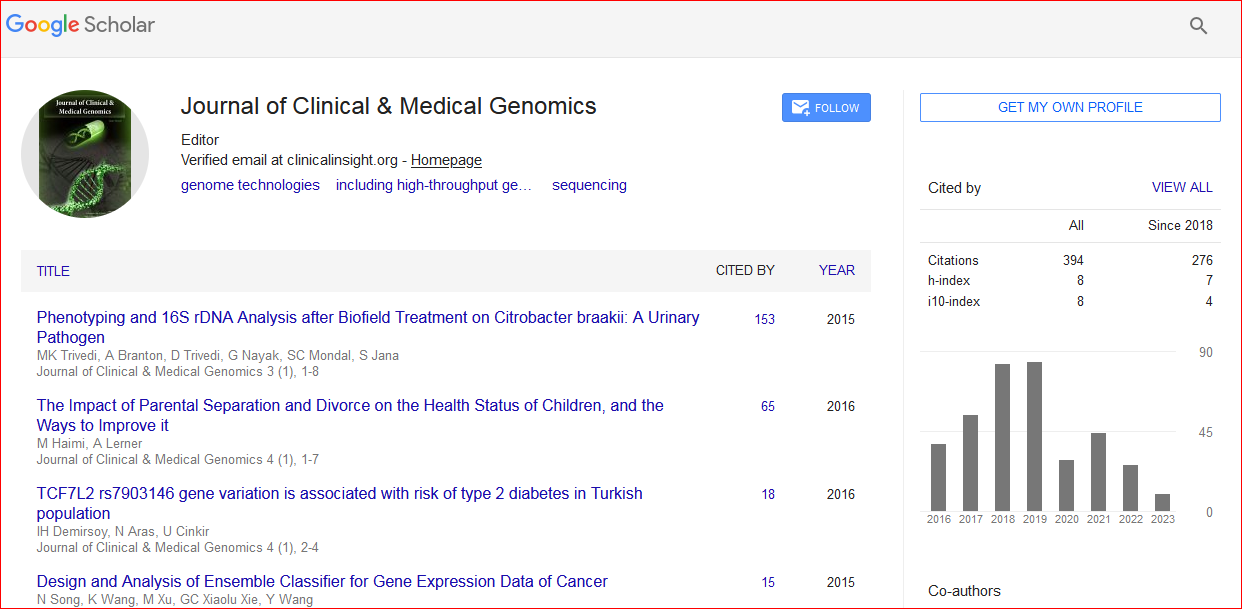
Journal of Clinical & Medical Genomics received 391 citations as per Google Scholar report