Case Series - (2022) Volume 7, Issue 4
Received: 05-Sep-2022, Manuscript No. JFM-22-74904;
Editor assigned: 07-Sep-2022, Pre QC No. P-74904;
Reviewed: 19-Sep-2022, QC No. Q-74904;
Revised: 24-Sep-2022, Manuscript No. R-74904;
Published:
30-Sep-2022
, DOI: 10.37421/jfm.2022.7.175
Citation: Ernan, Heff. “Advances in Suicide Prevention.” J Forensic Med 7 (2022): 175.
Copyright: © 2022 Ernan H. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
First responders are crucial in helping people who are experiencing suicide thoughts and directing their care. Examine current care pathways and models of care that may be employed for individuals who have come to the notice of first responders and are experiencing a suicide crisis.
In addition to conducting a scoping study of the academic and grey literature published between 2009 and 2019, experts, service providers, and people with lived experience were consulted.
Search results showed 703 studies. One personal letter and 23 publications from the grey literature and peer reviews were deemed appropriate for inclusion. 22 programmes were covered by six models, which were found. No papers that specifically addressed care pathways could be found. The utilisation of hospitals and police detentions were decreased when co-responder and safe haven models were used. Models of aftercare have been linked to greater wellbeing and a lessening of symptoms. Service users gave excellent reviews to the co-responder, safe haven, and aftercare models. Studies measuring the effect on longer-term suicidality are lacking.
A lack of comparability due to the variability of studies and their designs caused by the inclusion criteria's broadness. Few research used measurement techniques that were standardised, which made it harder to draw reliable findings.
Many innovative projects have the potential to help those in need who come in contact with first responders.
Suicide prevention • Suicide crisis • Suicide note.
Approximately 700,000 individuals worldwide die by suicide each year, which is a growing concern [1]. With 12.9 suicides per 100,000 people, suicide ranks as the 13th most common cause of death in Australia [2]. In addition, it is predicted that three Australians will try suicide in their lives for every 100 of them, and that four Australians will attempt suicide in a given year [3]. Furthermore, it is widely known that prior suicide attempts and suicidal ideation with intent are reliable indicators of future suicide [4]. According to one study, 81.8% of survivors of index attempts committed suicide within a year [4].
First responders, such as police and paramedics, are essential in assisting those in suicidal crisis and facilitating effective intervention and follow-up [5]. First responders in Queensland, Australia, get more than 200 suicide-related calls every day, according to the findings of a data linkage research, and over the three-year period from 2014 to 2017, there was an increase in suiciderelated calls of almost 25% across police and ambulance services [6].
Transport to a hospital emergency room has historically been the primary care pathway utilised by first responders in Australia for those who are experiencing or are at high risk of experiencing a suicide crisis (ED). Peerreviewed evidence indicating transportation to a hospital is the best course of action, however, is scant to nonexistent. There are considerable care barriers that patients with mental health issues, including suicide crises, who visit Australian emergency departments must overcome, according to recent reports. The idea that EDs are improper therapeutic contexts is also being expressed more frequently by those who have actually attempted suicide. An individual in crisis may be taken to a watch house for incarceration if there are no other suitable options or if they have also committed an offence.
The best way to help someone out of a crisis and stop further suicide attempts is through tailored, efficient treatments that can be given during or right after the initial response. First responders in Australia today have few alternatives to help people in need, especially after hours, and are further constrained by the catchment region the person lives in.
This scoping assessment looks into the choices that first responders may have to assist in providing care for someone who is experiencing a suicidal crisis. The successive interactions that people experiencing a suicide crisis have or may have with first responders and healthcare professionals are defined as care pathways in the paper [7].
In addition to consulting with well-known specialists and snowballing from the initial corpus of knowledge, a database search of peer-reviewed literature and grey literature was carried out. The PRISMA guidelines for systematic reviews served as a guide for the literature search. Suicidal phrases included "crisis," "care," "mental health," and "prevention," while terminology for models of treatment included "police," "first responder," "model of care," "coresponder," "suicidal sanctuary," "safe haven," and "alternative to admission." The search was restricted to English-language items that had been published over a ten-year period. Clinical expertise and consultation with recognised experts served as the basis for the grey literature search. For each of the identified models, peer-reviewed or published assessments were sought; this included getting in touch with service providers directly to learn about any published or unpublished materials.
There were 703 documents found in all. Twenty-three peer-reviewed and grey literature studies covering six models and one software that used human communication to collect data met the criteria for inclusion. The findings involved two systematic studies, 16 programmes that had formal evaluations published, and 6 programmes that did not.
Following is a description of six models that were found in the literature and cover 22 programmes.
Model 1: N=9 correspondents. A medical professional can be contacted right away for advice or co-responds with the police or ambulance. In order to free up first responder crews to resume their on-the-road responsibilities, the co-responder conducts mobile assessments and/or takes over the care of a person experiencing a suicide crisis.
Model 2: Time-limited and structured brief contact interventions, N=1, with a sympathetic response.
Model 3: Safe havens (brief stays): N=4. Safe, comfortable settings are a substitute for ED.
Model 4: Blended models, N=1, with high-tech call centres, round-theclock mobile crisis teams, and crisis stabilisation retreats/programs.
Model 5: Programs for Aboriginal and Torres Strait Islander people; N=2; culturally appropriate crisis solutions.
Model 6: Post-ED programmes that offer follow-up: N=5. The engagement has a time limit, and connections to other services are made. These initiatives could be changed to connect first responders with aftercare services immediately [8].
In this article, six models for 22 programmes that provide treatment to those in suicidal crises were identified. Reduced hospital utilisation and fewer police detentions were linked to the co-responder and safe haven models. Three of the five programmes' aftercare models, which used psychological assessments, demonstrated better client wellbeing and symptom reduction. Service users gave the co-responder, safe haven, and aftercare models positive reviews. Conclusions about the efficacy of blended models, culturally relevant crisis interventions, and brief contact treatments require more data.
The assessment noted compassionate answers that service users said saved their lives, despite shortcomings in the implementation and measurement of effectiveness. There were also suggestions to broaden, alter, or enhance existing models and programmes, such as allowing coresponders to work longer hours and allowing them to use crisis centres rather than EDs. In order to ascertain whether these programmes have a good effect on suicidality (ideation/behavior) and other outcomes professed to arise from them, as well as to identify which components matter to prevent suicidality and suicide in the long run, more research is necessary. Future service planning and implementation in the care of persons experiencing suicidal crisis should benefit from the findings of such studies.
Google Scholar, Crossref, Indexed at
Google Scholar, Crossref, Indexed at
Google Scholar, Crossref, Indexed at
Google Scholar, Crossref, Indexed at
Google Scholar, Crossref, Indexed at
Google Scholar, Crossref, Indexed at
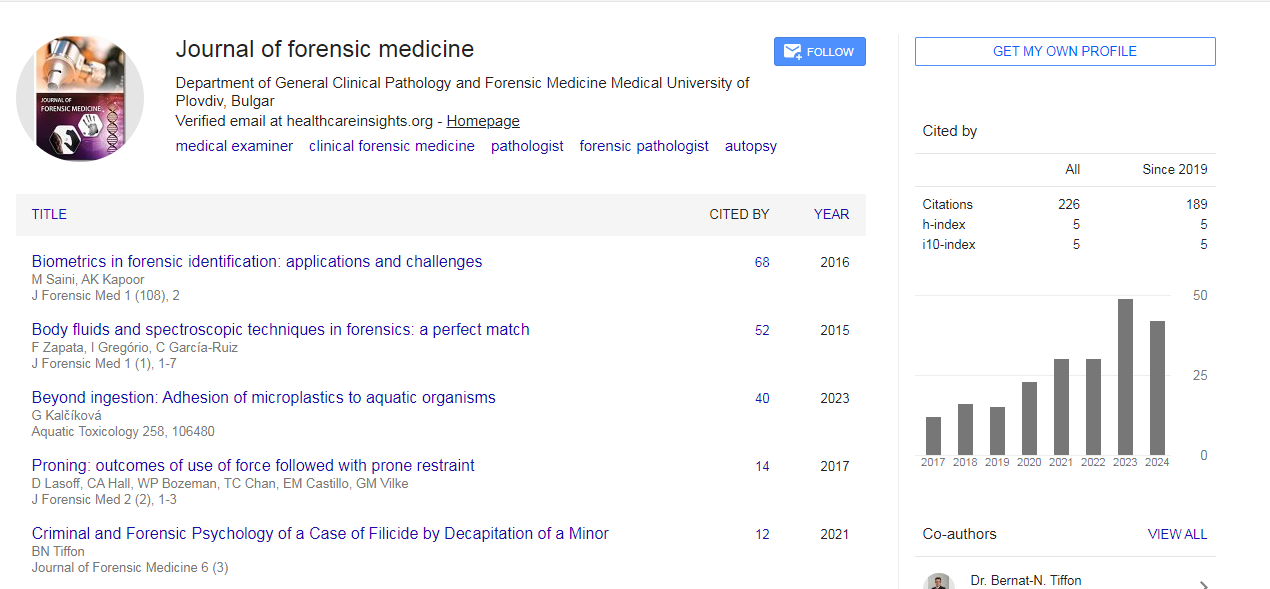
Journal of Forensic Medicine received 165 citations as per Google Scholar report