Kate Ball
Statement of the Problem: The concept of empathy in psychiatry infers an understanding, concern or interest in a person’s emotional state or experience. The experience of psychosis that usually precedes schizophrenia is often frightening; destabilizing a person’s sense of self and confidence in reality. Empathic action calls for ways to diminish the likelihood of a person experiencing psychosis. Methodology & Theoretical Basis: The current research tests the theory that vulnerability to developing this type of psychosis can be identified by an early-screening-tool (Schizophrenia-Traits-Questionnaire, STQ) in teenage, in a second stage of development by Flourish Australia. Originally developed in a PhD by the author, it is based on the neurodynamic/ psychobiological theory of Robert Miller. Originally, 600 adults participated in the STQ to test both the theory and its power to predict whether someone would fit into the schizophrenia category or not. The current research trial is on teenagers.
Findings: The factor analysis supported the underlying theory and thirteen (13) of the items in combination, in the original sample, accurately predicted schizophrenia to 85% accuracy with no mention of psychotic symptoms. With early-detection and the appropriate education and resources, not only can the STQ potentially stop a psychotic episode from occurring, it also identifies the types of occupations to avoid, to prevent being overwhelmed by stimuli/environments that challenge.
References 1. Miller R (2008) A Neurodynamic Theory of Schizophrenia and Related Disorders. Lulu Press, Raleigh, North Carolina. 2. Fukushima J, Chiba T, Tanaka S, Yamashita I and Kato M (1988) Disturbances of voluntary control of saccadic eye movements in schizophrenic patients. Biol Psychiatry; 23: 670-677. 3. Henik A and Salo R (2004) Schizophrenia and the stroop effect. Behavioral & Cognitive Neuroscience Reviews; 3: 42-59. 4. Nieuwenstein M R, Aleman A and de Haan E H (2001) Relationship between symptom dimensions and neurocognitive functioning in schizophrenia: a meta-analysis of WCST and CPT studies. Wisconsin Card Sorting test. Continuous Performance Test. Recent focus on early detection and intervention in psychosis has renewed interest in subtle psychopathology beyond positive and negative symptoms. These are self-experienced subclinical disturbances termed basic symptoms (BS). The phenomenologies of BS and their development in the course of psychotic disorders will be described. Diagnosis, treatment, and research studies of psychosis have focused mainly on its cardinal positive and negative symptoms. However, the current attention on prodromal phases of the illness has generated renewed interest in the early subtle, self-experienced changes in mentation that have been observed and described since Kraepelin's articulation of dementia praecox. The most thorough description of these symptoms is provided within the framework of the basic symptoms (BS) concept developed by the German psychiatrist Gerd Huber. BS are subtle, subjectively experienced subclinical disturbances in drive, affect, thinking, speech, (body) perception, motor action, central vegetative functions, and stress tolerance. They can occur and have been reported in every stage of the illness, ie, in the prodrome to the first psychotic episode, in prodromes to relapse, in residual states, and even during psychotic episodes per se.
By definition, BS are different from what is considered to be one's “normal” mental self. Being subjective, they remain predominately private and apparent only to the affected person. They are rarely observable to others, although a patient's self-initiated coping strategies (including avoidance strategies and social withdrawal) in response to his/her BS may be recognizable to others. Being self-experiences, BS differ from negative symptoms as they are currently understood, ie, as functional deficits observable to others. BS is also distinct from frank psychotic symptoms that are experienced by the patient as real, normal thinking, and feeling. In contrast, BS is spontaneously and immediately recognized by the affected person as disturbances of his/her own (mental) processes. Insight that something is wrong with one's thinking is present, yet some experiences might be so new and strange that they remain nearly inexplicable. The rare, highly introspective person may be able to articulate what is happening, but any detailed description of these experiences usually requires help in the form of guided questioning. The ability to experience BS with insight and to cope with them often attenuates with progressive illness and emerging psychotic symptoms but is restored upon remission. Thus, an evaluation of BS is often hindered by acute and/or prominent psychotic symptoms.
In Anglo-American psychiatry, 2 researchers, James Chapman and John Varsamis, described self-experienced symptoms like BS in the 1960s and 1970s without exploring them in as much detail as Huber and colleagues. Recently, BS emphasizing anomalies of self-awareness have been described by Josef Parnas. BS is an integral part of the psychoses and can appear throughout various stages of the disorder. Currently, BS is mainly employed in the early detection and preventive intervention of psychosis. In clinical practice, the most important feature of BS is that they are experienced and reported as abnormal and burdensome by the patients themselves. As such, they are appropriate to describe in awareness and information campaigns of psychosis to promote early detection and indicated prevention. They should also be described to patients in remission from psychosis as representing early signals of a risk for relapse. BS is also important signals of the need for rehabilitation in residual, post psychotic states. They support a more complete description of the degree of remission beyond positive and negative symptoms. In this, BS can be used for titrating adequate combinations of pharmacological, psychological, and rehabilitative interventions. BS were regarded as the earliest subjectively experienced symptoms of psychosis and the most immediate symptomatic expression of the neurobiological correlates of the illness —thus the term “basic.” According to the original concept, (early) symptoms of psychosis occur in 3 developmental forms: “uncharacteristic” BS affecting mainly drive, volition, and affect, as well as concentration and memory (level 1); “characteristic”, qualitatively peculiar BS, especially of thinking, speech, (body) perception, and motor action (level 2); and psychotic symptoms
Finally, a patient's encounters with and motivations for treatment may be improved by relating therapeutic strategies to phenomena that are clearly recognized as subjectively burdensome symptoms. The BS concept can also educate patients and their families about the expressions of psychosis and support them in acquiring a deeper understanding of the expected vicissitudes of their illness, an important step in the process of stripping “madness” of some of its intractability and terror. Finally, consideration of BS may help the therapist in achieving insight into a patient's failure to master some problems that might be a reaction to BS
PDFShare this article
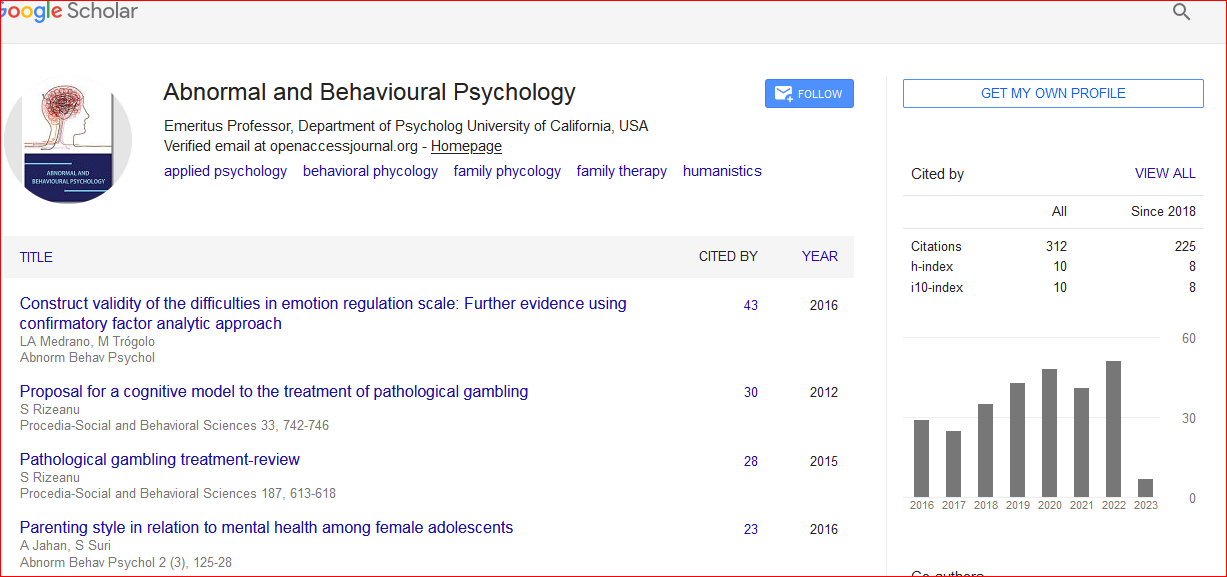
Abnormal and Behavioural Psychology received 361 citations as per Google Scholar report