Abhinav Joshi
Most of the times the presentation of a psychiatric illness is very different from the text book description. On one hand, the symptoms of the illness may show symptoms of different psychiatric illness and at other times the symptoms are too vague to label them under a single clinical diagnosis. There are various indications of giving mood stabilizers and anti-psychotics (some of them also already have mood stabilizing properties and also given for management). The common indications are bipolar disorder, Schizoaffective disorder. And, if the patients have additional diagnosis of treatment resistant anxiety or depression, the reasons for concurrent use may range from augmentation of effect of one medication to target particular symptom or receptor. Most of the times the concurrent use has a beneficial value but at other times it may lead to unexpected side effects, generally because of altered pharmacokinetics and pharmacodynamics. In this case report we will try to present a case of Schizoaffective disorder and the effect of using Aripiprazole and Sodium Valproate together on patient's symptoms.
Presently in its third decade of distribution, Psychological Medicine is a main worldwide diary in the field of clinical psychiatry and the essential sciences identifying with it. Each issue contains unique articles revealing key examination being attempted around the world, along with more limited publications by recognized researchers and a significant book audit area.
It is turning out to be progressively certain that we can improve clinical consideration by giving more consideration to mental parts of clinical evaluation and treatment. The examination and practice of such factors is regularly called mental medication. Problems that are customarily, and maybe misleadingly, named mental are exceptionally predominant in clinical populaces. In any event 25-30% of general clinical patients have existing together burdensome, nervousness, somatoform, or liquor abuse problems. A few components represent the co-event of clinical and mental issues.
Another explanation behind mental medication is the pervasiveness of side effects that are unexplained by illness. Albeit physical indications represent the greater part, all things considered, to specialists, at any rate 33% of these manifestations remain therapeutically unexplained.
Mental medication is significant in the administration of every one of these issues; both psychotropic prescriptions and psychological conduct medicines have demonstrated compelling in the treatment of basic physical manifestations and conditions in various investigations all in all practice.
Although such medicines have customarily been viewed as mental, they are likewise advantageous in patients without obvious mental problems. Nations on the two sides of the Atlantic have far to go in creating mental medication, the gorge in America among clinical and mental consideration is especially profound.
Mental medication doesn't mean relabelling all such patients as mental. Numerous patients want to have these issues viewed as clinical and conceptualized regarding synapse unevenness or a practical real unsettling influence.
Attendant mental pain is best outlined as far as being an outcome instead of a reason for constant physical manifestations. Untimely endeavors to reattribute physical objections to mental instruments might be seen by the patient as dismissal. An all the more etiologically nonpartisan yet mentally advanced methodology that at first spotlights on suggestive treatment, consolation, enactment, and rebuilding of capacity has demonstrated more compelling.
Mental medication may likewise be conveyed in some creative manners. Promising information exist for social intercessions led outside the specialist's office, including case the board by phone, intellectual conduct treatment given through a PC, bibliotherapy - self investigation by patients and home visits.
Mental medication likewise improves results. The advantages of treating basic physical manifestations and mental pain successfully in clinical patients incorporate not just improved personal satisfaction and social and work working, yet in addition more prominent fulfillment with respect to patient and specialist and decreased utilization of medical care administrations.
Aripiprazole, characterized as a third-age antipsychotic drug (APD) because of its one of a kind pharmacological profile, speaks to an imaginative helpful device for major mental issues. Its modulatory properties on various synapse frameworks (see area: Overview of the pharmacological profile) feature a medication with a wide pharmacological profile and clinical viability in the intense and long haul therapy of various psychopathological conditions, as exhibited in clinical preliminaries. Second-age antipsychotics have been demonstrated to be similarly, or more, viable than exemplary antimanic operators, for example, lithium and valproate, in the treatment of madness related with bipolar turmoil.
Sodium valproate and related arrangements have as of late gone through administrative audit following worry about impacts on the unborn youngster and specialists' inability to convey hazard. The issues are more extensive. Valproate is abused in psychiatry dependent on the bogus recognition that 'usability' likens to preferable wellbeing over other options. Valproic corrosive can disturb principal physiological cycles, the outcomes of which are ineffectively perceived and little talked about in the mental writing. Valproate might be helpful in few patients with bipolar confusion however current recommending designs are uncalled-for. Discernment needs to change.
Background:
The interaction between anti-psychotics and mood-stabilizers do not follow a particular pattern. Some increase and others decrease the concentration of each other leading to positive or negative therapeutic effects. It is important to understand the drug-drug interaction when administering antipsychotics and mood stabilizers for clinical safety and avoid potential preventable side effects.
Case Presentation:
Madam T is a 32-year-old, Chinese lady, who is a known case of Schizoaffective disorder since 2008. Over the years, she was trialed on various psychotropics but was stopped due one or another reasons: Olanzapine (weight gain), Risperidone (tremors), Haloperidol (possible oculogyric crisis), Valproate (weight gain), Sulpiride (not effective). She presented to the emergency room for being paranoid and poor social support and some concerns about homicidal delusions. She also exhibited her relapse signature including paranoia, auditory hallucinations, thought control symptoms and believe to communicate via telepathy with others. She was convinced that she was pregnant despite urine pregnancy and blood HCG test to be negative. She was also noted to be irritable, agitated and pacing around in the ward. She insisted for her personal belongings to be returned and also snatched the staff nurse's access pass and kept her inside her underwear, only to give it back when her demands were met. When she was tried to admit her in the psychiatric ward, she locked herself in the toilet and stripped naked. She needed security activation as well as chemical and physical restraints at this point of time. In the ward she displayed loosening of associations, delusion of grandiosity, hyper-religious ideas, labile mood and no insight into her illness. Though, initially she refused to take any medications, subsequently agreed to take oral Aripiprazole 30 mg OM. She seemed to start settling after starting Aripiprazole with decreasing severity of disordered thoughts, hallucinations and improving insight. She was switched to IM Aripiprazole 400 mg in view of history of non-adherence to treatment. At the same time, she was started on PO Valproate in view of affective symptoms. However, her condition rapidly deteriorated with increase in manic and psychotic symptoms. Valproate was stopped and she was given IM depot Zuclopenthixol along with top up dose within a week (100 mg), but to no improvement. She was also tried on Trifluoperazine 10 mg BD, however no response despite adequate titration. Eventually she was started on Clozapine 200 mg ON. There was some improvement in sleep but she was still floridly manic and psychotic. In view of treatment resistance and prominent affective symptoms, she was started on right unilateral electroconvulsive therapy. She responded fairly well to electroconvulsive therapy though was till mildly manic at the time of discharge.
Discussion: There is no published metanalysis on the interaction between antipsychotics and mood stabilizers. I have tried to summarize individual drug-drug interactions between mood stabilizer and antipsychotic. The following tables summarizes the effects of some interactions between anti-psychotics and mood stabilizers.
Share this article PDF
PDF
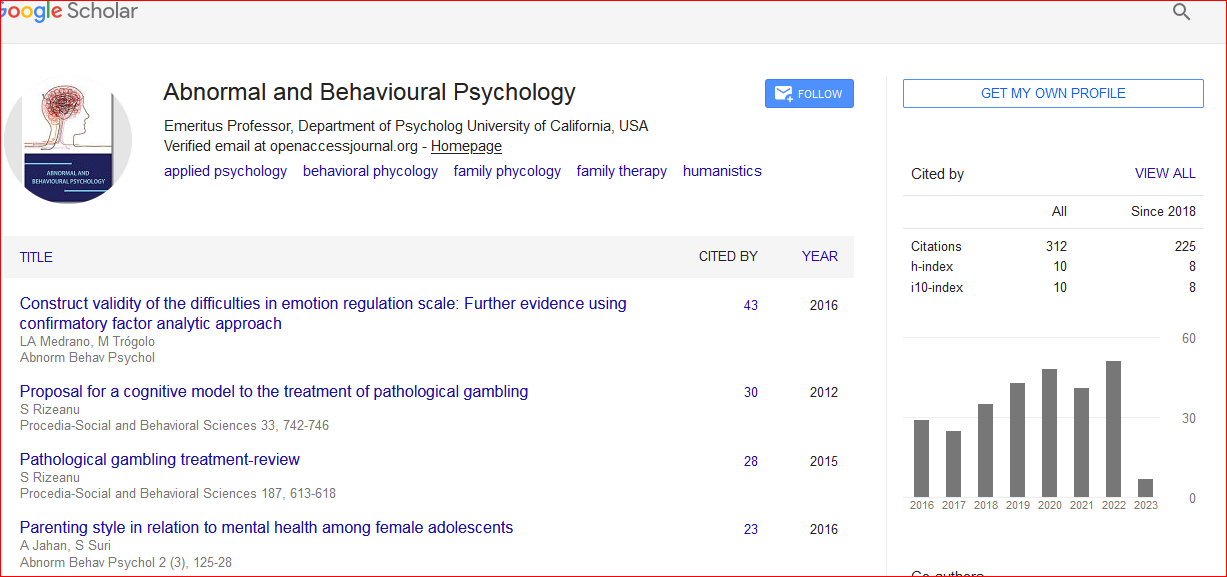
Abnormal and Behavioural Psychology received 361 citations as per Google Scholar report