Commentary - (2025) Volume 13, Issue 2
Received: 01-Dec-2025, Manuscript No. JCMG-25-165761;
Editor assigned: 03-Apr-2025, Pre QC No. P-165761;
Reviewed: 17-Apr-2025, QC No. Q-165761;
Revised: 22-Apr-2025, Manuscript No. R-165761;
Published:
29-Apr-2025
, DOI: 10.37421/2472-128X.2025.13.331
Citation: Chen, Clinton. “Leveraging Polygenic Risk Scores to Optimize Pharmacogenomics and Drug Response Prediction.” J Clin Med Genomics 13 (2025): 331.
Copyright: © 2025 Chen C. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Emerging evidence suggests that complex drug responses often involve the interplay of multiple genetic variants across the genome, each contributing modestly to the phenotype. This polygenic architecture mirrors what has been observed in complex diseases like diabetes, cardiovascular disease, and psychiatric disorders. Consequently, researchers have begun to explore the utility of Polygenic Risk Scores (PRS)—aggregated measures of genetic liability calculated from Genome-Wide Association Study (GWAS) data—as tools to capture this complexity. PRS are typically derived by summing risk alleles across many Single-Nucleotide Polymorphisms (SNPs), weighted by their effect sizes estimated from GWAS. The result is a single quantitative measure that reflects an individual's inherited predisposition to a given trait or outcome. While PRS have primarily been applied to disease risk prediction, their application to pharmacogenomics represents a compelling and underexplored domain that could significantly advance precision medicine [1].
Integrating PRS into pharmacogenomics offers several conceptual and practical advantages. First, PRS can capture a broader spectrum of genetic influences than traditional single-gene pharmacogenetic markers. For many drugs, especially those used in treating multifactorial conditions, response and adverse effects are influenced by numerous small-effect variants rather than a few high-impact ones [2]. For example, the response to statins, antidepressants, and antihypertensives is only partially explained by known pharmacokinetic and pharmacodynamic genes. PRS can complement these markers by accounting for additional genomic contributions, including those related to underlying disease susceptibility or relevant physiological pathways. In this way, PRS can serve as an integrative measure that bridges pharmacogenomics and disease genomics, providing a more comprehensive picture of individual variability in drug response [3].
Second, PRS can be used to stratify patients by their likelihood of responding to a particular therapy or experiencing side effects. This stratification can inform drug selection, dosing strategies, and monitoring plans [4]. For instance, in psychiatric treatment, where drug efficacy is often unpredictable and adverse effects are common, PRS for schizophrenia, depression, or bipolar disorder could potentially identify individuals more likely to respond to specific antipsychotics or antidepressants. Pilot studies have already indicated associations between higher schizophrenia PRS and greater benefit from clozapine, an antipsychotic reserved for treatment-resistant cases. Similarly, in oncology, PRS for breast cancer subtypes may one day help determine which patients are likely to benefit from hormone therapy versus chemotherapy. These applications underscore the utility of PRS as predictive biomarkers for therapeutic decision-making [5].
Google Scholar Cross Ref Indexed at
Google Scholar Cross Ref Indexed at
Google Scholar Cross Ref Indexed at
Google Scholar Cross Ref Indexed at
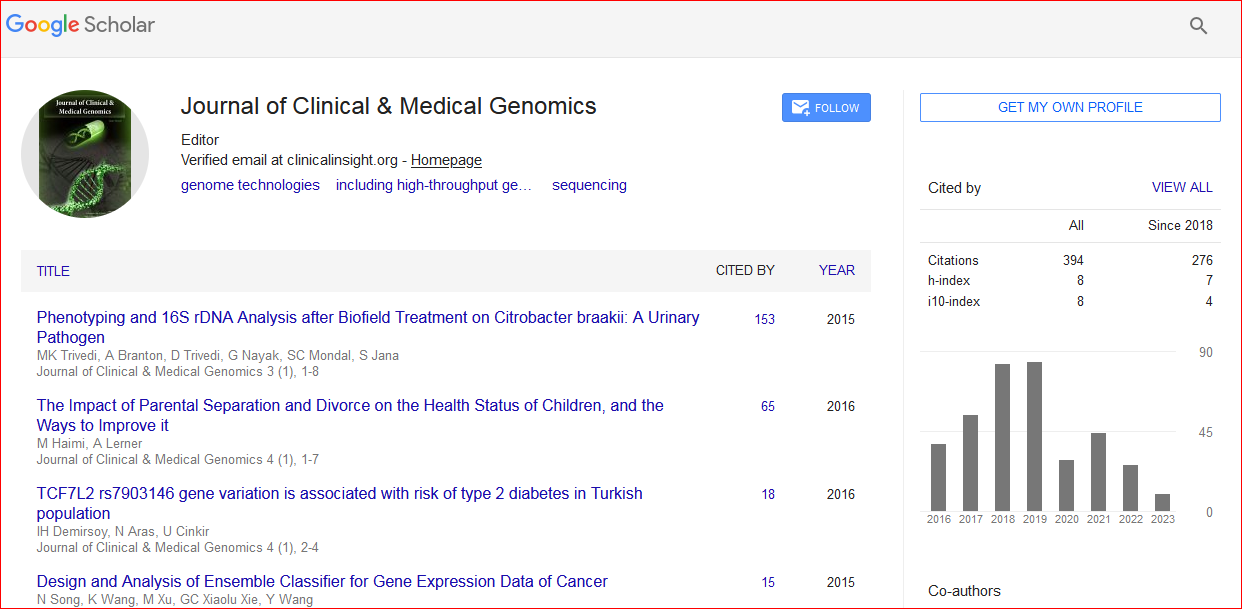
Journal of Clinical & Medical Genomics received 391 citations as per Google Scholar report